Hernias
Surgery to Repair Hernia
Information for Patients
What is a Hernia?
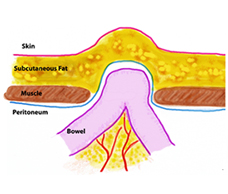
A Hernia is an out-pouching of intra-abdominal contents through a defect, or hole in the muscle. The abdominal muscles and bones of the pelvis prevent abdominal contents from drooping out under normal circumstances. The skin and fat below the skin do not provide any strength and stretch if there is a hernia present.
Hernias can occur anywhere in the abdomen, but most commonly occur at weak points where a small tear can start, and enlarge over time. The common weak points are
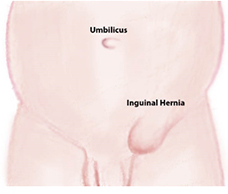
- Inguinal – This is the most common in men, the weak point is near where the spermatic cord courses through the muscle
- Femoral – Here the weak point is where the blood vessels to the thigh and leg pass through at the bottom of the pelvis
- Umbilical – Hernias around the belly button are common and often present as an ‘outie’ type umbilicus
- Incisional – Scar tissue after previous surgery is weaker than the surrounding muscle and can tear to form a hernia
- Epigastric – Some people get hernias in the region between the belly button and the breast bone
- A history of heavy lifting
- Male Sex
- Obesity
- Chronic cough, constipation or urinary retention
- Previous surgery
- A lump that comes and goes and is more prominent on standing or straining
- Pain, discomfort or 'dragging' sensation at the site
- Incarceration or strangulation (see below)
- Incarceration occurs with a long term (chronic) hernia where the contents come out and stay out and are unable to be pushed back in. This often causes discomfort or mild to moderate pain but not severe pain.
- Strangulation is where in the short term the contents come out and can not be pushed back in, and where the defect causes such pressure on the blood vessels that the contents are starved of blood supply. This causes swelling, and severe pain. This is an emergency and warrants prompt attention at hospital.
- Hernia recurrence. No matter what method of repair is used there is a small lifetime risk of the hernia recurring. Unfortunately, no repair is as good as the original.
- Nerve injury. Applies particularly for open inguinal hernia repair. May occur as numbness near the scrotum, or a chronic pain (rare) running down the thigh or testicle.
- Injury to the testicular artery. The artery supplying the testicle runs with inguinal hernias and is extremely rarely injured during the repair. It would tend to present as a swollen, very painful testicle that would gradually shrink to less than its normal size, or require removal because of pain.
- Wound infection.
- Infected mesh, while rare needs further surgery to remove it!
- Clots
- Allergic reactions
- Heart troubles
Predisposing factors
It is not always possible to identify the time when a hernia started, although sometimes that is the case. Hernias are often associated with either weak muscles or raised abdominal pressure (or both).
Frequent features are:
Symptoms of hernia
There are frequently no symptoms of hernia. When present, the common symptoms are:
Complications of Hernias
Hernias do not repair themselves. Over time hernias tend to get bigger as the defect in the muscle stretches to allow more abdominal contents to slip in and out. As time goes on there is a risk that the hernia will develop a complication.
Who needs a hernia repair?
Patients with hernias, who are fit enough to undergo surgery should have hernias repaired before complications occur. Patients with strangulated hernias require urgent repair.
What tests are done?
Most commonly hernias are diagnosed clinically by your doctor. Sometimes ultrasound and/or CT scans can help rule out other causes of symptoms and diagnose the hernia. Tests to ensure safety of anaesthesia are performed according to age group and risk factors.
How is the hernia repaired?
The principle of hernia repair is to reduce the contents back into the abdominal cavity and close the muscle. There are various techniques for closing the muscle and your surgeon will discuss the options and make recommendations in your instance. In general small defects can be closed with a simple stitch technique, whereas larger defects are best dealt with by placing an artificial mesh over the hole, with the advantage that a large area is covered, and there is no tension on the repair that would encourage stitches to pull through and lead to a recurrence.
Can it be repaired with laparoscopic (keyhole) surgery?
Yes, this is the most common method of repair, although it is not suitable for everyone. The advantage of laparoscopic repair is that there is less pain and therefore a quicker return to normal, and sporting activities.
The postoperative course
The post operative course is different for each person. Most patients go home on the day of or the day after surgery.
Sutures are dissolving and buried, dressings can stay on for 7 days.
A follow-up appointment is made for 3 weeks after surgery. You may eat and drink normally, and walk around straight away. Heavy lifting and vigorous sports should be avoided for 6 weeks after the surgery.
Serious complications after hernia surgery are rare
Complications of hernia surgery include (but not limited to)
FAQs
Will I be able to go to the gym / lift heavy objects again?
Yes, while there will always be a risk of another hernia, the risks are small after a mesh hernia repair. Dr Crawford will inform you when you are ready to go back to these activities (usually at least 6 weeks after surgery).
What should I do if the hernia strangulates before surgery can be scheduled?
If the hernia suddenly becomes swollen and painful or has a red appearance, then you should lie down and try to gently push it back. If this works you should contact your doctor as soon as possible. If this does not work within 30 minutes, then you should go immediately to hospital.
Does the mesh stay in permanently?
Yes. In general, the mesh is made of a polypropylene or polyester material that blends with your muscle by promoting scar tissue. It reinforces your muscle and is intentionally not dissolvable. It is very rare for the mesh to need to be removed, but if it were to get infected it should be removed with another operation.
You will need the Adobe Reader to view and print these documents. ![]()
 Meet
Meet







