Laparoscopic & Hepatobiliary Surgeon
Speciality
The Liver makes bile and excretes it into a long tube (the bile duct) that joins the first part of the bowel. Bile is a salty solution that helps to make fats that we eat dissolve in water (so that we can absorb them). When there is no fat in the gut, the bile is stored in the gallbladder. When we eat fat, a chemical messenger makes the gallbladder contract, squeezing bile into the gut. Around 1 in 10 adults have gallstones. These begin as small crystals in the gallbladder and grow over time. These stones can cause irritation to the gallbladder, particularly when fat is consumed, causing pain and nausea (biliary colic).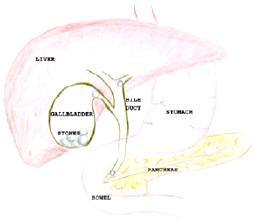
We are unsure why certain people get stones and others don’t. Some factors that have been found to be associated with gallstones are:
Biliary colic is the most common symptom of gallstones. It is pain or discomfort, in the upper abdomen, usually bought on by food (especially rich food). It lasts for minutes to hours, until the gallbladder relaxes.
Severe Complications of Gallstones
Acute cholecystits is a severe infection of the gallbladder. It begins like biliary colic, but fails to improve, and is associated with fever. Acute cholecystitis will usually settle with antibiotics in hospital. If it does not settle, then urgent surgery is required.
If stones escape from the gallbladder into the bile duct, they may cause partial or complete blockage of the bile duct with infection and jaundice.
This is an inflammation of the pancreas which is a digestive organ at the back of the abdomen. Small gallstones that have escaped from the gallbladder into the bile duct can pass past the pancreas and cause it to become inflamed..
Patients with any of the severe complications of gallstones should have a cholecystectomy. Patients with gallstones and symptoms should have a cholecystectomy, before the development of severe complications. Occasionally patients without gallstones, who have significant symptoms, will require a cholecystectomy (once other causes have been ruled out).
Most patients have gallstones diagnosed by ultrasound. The ultrasound will also show the width of the bile duct, which will help to determine the risk of stones outside the gallbladder. Routine blood tests including liver function tests.
The most common method of removal of the gallbladder is with laparoscopic (keyhole) surgery. A small cut is made under the umbilicus (belly button). Through this a camera is placed, and gas is instilled. 2 or 3 other small cuts are placed in the upper abdomen, through which instruments are introduced to dissect free the gallbladder. An x-ray (cholangiogram) will be performed through the gallbladder (cystic) duct to rule out stones in the main duct.
The cystic duct and cystic artery are then clipped with permanent titanium clips. These do not cause any long term problems or interfere with MRI. The gallbladder is then removed from its attachment to the liver and removed in a plastic bag.
The post operative course is different for each person. Most patients stay one night in hospital. 1 week off work.
Sutures are dissolving and buried, dressings can stay on for 7 days.
A follow-up appointment is made for 3 weeks after surgery. You may eat and drink normally after a day or two.
Serious complications after gall bladder surgery are rare.
FAQs
Yes, most patients will tolerate a normal diet afterwards, and there are no restrictions.
No, removing the stones would be more dangerous than removing the whole gallbladder and methods to dissolve them or blast them make the serious complications more likely.
No, the gallbladder is largely redundant, and the bile ducts will store all the bile necessary for healthy function.
![]() Laparoscopic Cholecystectomy (Removal of the Gallbladder)
Laparoscopic Cholecystectomy (Removal of the Gallbladder)